Retake
A18) Abdominal pain and distension with history of constipation
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with abdominal pain.
- Review the DDx considerations in a patient with abdominal pain.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a patient with abdominal pain.
History
A 35-year-old male with a history of diplegic cerebral palsy and chronic constipation presents to the emergency department with a 12-hour history of severe, colicky abdominal pain, abdominal distention, and vomiting. He reports not having a bowel movement for the past week, which exceeds his usual pattern of constipation. Additionally, he has been unable to pass gas during this time.
Physical Exam
BP: 105/77, HR 105, RR 14, Temp 98°F, O2 saturation 99% on room air
General: Alert and cooperative, though appearing fatigued and uncomfortable.
HEENT: Dry mucous membranes.
Cardiovascular: Tachycardic, regular rhythm, no murmurs, rubs, or gallops. Bilateral pulses 1+, capillary refill time of 3 seconds.
Abdominal: Markedly distended, tympanic, with severe tenderness in the left lower quadrant. No rebound tenderness, rigidity, or guarding. Digital rectal exam reveals an empty rectal vault and no frank blood.
Neurological: Motor strength 4/5 in upper extremities and 3/5 in lower extremities (baseline). Patellar reflexes 3+.
Labs
WBC (White Blood Cell count): 12,000/mm3 (Normal range: 4,500-11,000/mm3),
Sodium (Na): 132 mmol/L (Normal range: 135-145 mmol/L),
Potassium (K): 3.2 mmol/L (Normal range: 3.5-5.1 mmol/L),
Chloride (Cl): 98 mmol/L (Normal range: 96-106 mmol/L),
CO2 (Bicarbonate): 18 mmol/L (Normal range: 22-30 mmol/L)
Provisional Diagnosis
Select the Dx you believe is most appropriate
The patient presents with a history of chronic constipation secondary to diplegic cerebral palsy, along with severe colicky abdominal pain, abdominal distention, vomiting, and obstipation. These symptoms are more consistent with bowel obstruction.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
In this patient, there are no signs of bowel ischemia, such as rebound tenderness, rigidity, or guarding, which would indicate a need for emergent surgery. Furthermore, the patient is hemodynamically stable. Therefore, although the patient requires urgent evaluation and management, immediate workup and management may not be necessary.
First Imaging Study
What is the first imaging study you will order?
In patients with suspected high-grade bowel obstruction, the most appropriate initial imaging modality is a CT scan of the abdomen and pelvis. CT scans are accurate in identifying the presence and cause of obstruction, and detecting the presence of complications, such as strangulation and ischemia. Additionally, CT scans can effectively guide patient management, triaging them into operative or nonoperative treatment groups based on the findings.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
CTAP with IV contrast
Which structures are dilated?
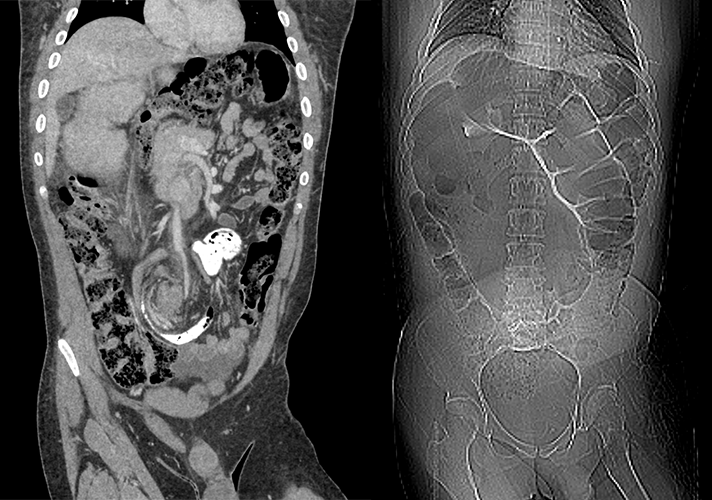
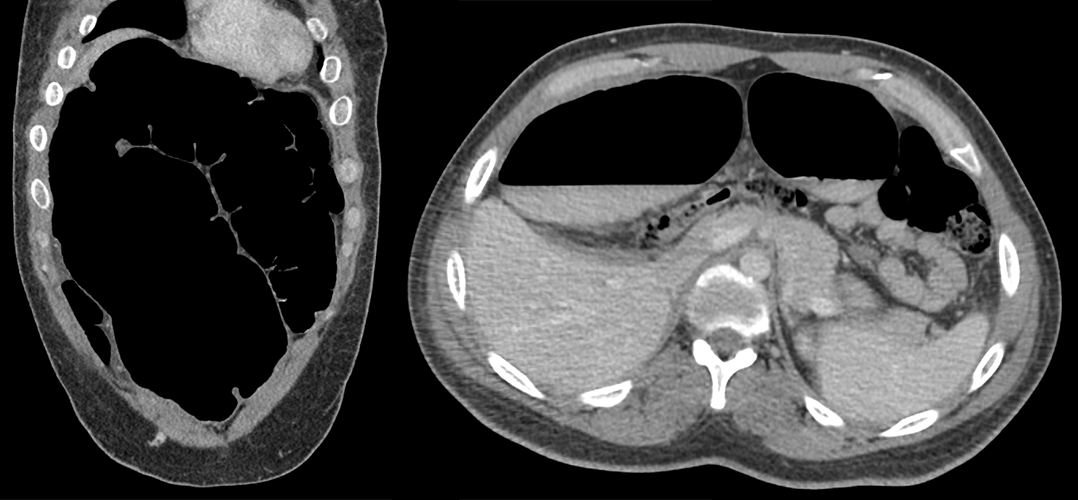
The imaging reveals a significantly distended large bowel, characterized by the presence of haustra. The scout film and coronal CT demonstrates the classic "coffee bean" sign, oriented towards the right upper quadrant. No plicae circulares indicative of small bowel dilation or intraperitoneal free air or pneumatosis intestinalis are observed.
What best describes the findings on the CT?
The root of the sigmoid mesocolon, the mesentery connecting the colon to the posterior abdominal wall, appears twisted into a spiral. This classic imaging finding, known as the "whirl sign," indicates a volvulus. In this scenario, the redundant sigmoid colon has twisted around itself at the base of the mesocolon.
There are signs of vascular compromise.
While twisting of the sigmoid colon around its mesocolon may eventually result in bowel necrosis, no evidence of such progression like pneumatosis, portal venous gas, or pneumoperitoneum is currently present.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is needed. Further imaging would not change the patient’s management.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient presents with a history of chronic constipation secondary to diplegic cerebral palsy, along with severe colicky abdominal pain, abdominal distention, vomiting, and obstipation. Imaging confirmed the presence of sigmoid volvulus.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
This patient should be evaluated urgently. Prolonged sigmoid volvulus can lead to bowel ischemia, necrosis, perforation, and sepsis.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient presents with a history of chronic constipation due to diplegic cerebral palsy, accompanied by severe colicky abdominal pain, abdominal distention, vomiting, and obstipation. Imaging reveals an enlarged large bowel with the "coffee bean sign" and "whirl sign," confirming a sigmoid volvulus. Initial management includes IV fluid resuscitation, maintaining NPO status, inserting a nasogastric tube, and consulting general surgery for sigmoidoscopy and potential detorsion of the volvulus or surgical intervention. IV analgesics should be administered, and IV broad-spectrum antibiotics should be provided to cover potential bacterial translocation or ischemic bowel. The patient's chronic constipation should be addressed, and a referral to a gastroenterologist for long-term management may be considered.
Lessons Learned:
- Sigmoid volvulus occurs when a redundant sigmoid colon twists around its own mesentery, creating an occluded bowel loop.
- Key risk factors include constipation (chronic constipation leads to sigmoid colon elongation, making it "redundant" and more likely to twist around its mesocolon), older age, male sex, and prior abdominal surgeries.
- Patients typically present with colicky abdominal pain, constipation, and distention, progressing to constant diffuse pain accompanied by nausea and vomiting.
- Vomiting and anorexia can cause dehydration, leading to hypotension, tachycardia, fatigue, hypochloremic hypokalemic metabolic alkalosis, hemoconcentration, and signs of acute kidney injury.
- Hemodynamic instability, leukocytosis, fever, and peritonitis may indicate bowel ischemia or perforation, necessitating emergency surgery.
- The preferred initial imaging study is a CT abdomen and pelvis with IV contrast. The classic "whirl sign" represents the twisted sigmoid mesocolon.
- If an abdominal X-ray is obtained, the classic "coffee bean" sign, oriented towards the right upper quadrant, represents the distended sigmoid colon.
- The large bowel can be differentiated from the small bowel by the presence of haustra, which do not extend completely across the bowel.
- Urgent management includes decompression using flexible sigmoidoscopy, with surgery warranted if signs of ischemia are present.
Socioeconomic Factors:
- Constipation often impacts institutionalized patients for various reasons. Therefore, they may be at a higher risk for sigmoid volvulus.
- Chagas disease, prevalent in tropical regions and among individuals with limited access to quality housing, can predispose people to sigmoid volvulus as it can lead to megacolon.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}